|
| |

 |
 |
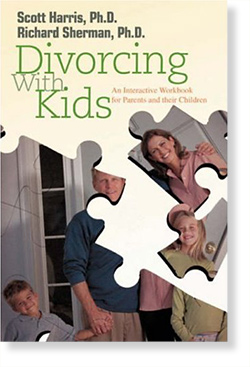
Divorcing with Kids: An Interactive Workbook
for Parents and their Children
by Richard Sherman, Ph.D. and Scott Harris, Ph.D.
This workbook will help parents and their children get through the painful process of separation and divorce. The author's approach is to give parents ways to assist taking care of their children's needs while not forgetting their own. Through a liberal use of examples and exercises, the goal is that both the parents and the children will gradually feel more hopeful and encouraged.
"This workbook is insightful and carefully crafted to help parents and their children navigate the emotions of divorce. I will be giving this workbook to each of my clients!"
—Marlo Van Oorschot, Attorney/Mediator, West Los Angeles
|
About the Authors
Richard Sherman, Ph.D., 2007 California Psychological Association President, has a clinical and consulting practice in Tarzana, California. He speaks on the impact of television and the Internet on families.
Scott Harris, Ph.D., clinical psychologist (Southern California), has a private practice and consults. He authored a parent’s guide, When Growing Up Hurts Too Much.
This workbook can be purchased through Amazon.com

RADIO
(Partial
list)

AirTalk with Host Larry Mantle
10-noon, Monday-Friday
How to Talk to Kids About War
March 19, 2003
KPCC FM, Pasadena, CA | http://www.scpr.org
>
Listen
Joining host Larry Mantle to discuss this, experts Dr.
Richard Sherman, a clinical and consulting psychologist,
and Betsy Brown Braun, a Child Development Specialist
and Parent Educator.
RADIO
Frequent on air contributor and producer, The Mark Isler Show
http://www.markislernow.com
TV
(Partial list)

EverQuest' Kills Cupid, February 10,
2003 | TechTV cable channel
Online role-playing game causes tension in some relationships
and has even broken up marriages.
By Becky Worley, Tech Live

Who'd have thought technology would ruin Valentine's
Day? But for Joy Barnes, the fantasy role-playing game
"EverQuest" put a serious damper on romance.
In fact, she says it killed her marriage.
Her husband was addicted to the game, she says, playing
up to 16 hours a day. And when it came down to choosing
between their marriage and the game, Barnes says her
husband chose the digital fantasy world and his crowd
of virtual friends.
"In a non-technological universe, he might have
been at a bar," Barnes said. "But this was
something he could roll out of bed and go into the other
room to [do], and [he could] talk to all of his friends
24 hours a day. It's different from a bar; that has
to close sometime."
But Barnes says she doesn't want to misrepresent the
game. She's a gamer herself. She even took up "EverQuest"
herself to play with her husband and hopefully find
some common ground. She says the game is great, but
she never had the desire to play for hours on end.
She eventually divorced her husband.
The game does lend itself to long hours of play. "EverQuest"
is an online role-playing game in which players become
mythical warriors who battle evil with the help of online
friends. A lot of endless chatting goes on, and many
complex social relationships evolve. And the game is
truly endless -- there's no big pay-off where you come
to the end of the experience.
Clinical psychologist Richard Sherman says the game
can take on a prominent role in the player's life.
"A person gets so hooked on these games that they
would rather spend time with the game, which becomes
in a sense their new lover, than with their own partner,"
he said.
Barnes says she felt abandoned because her husband would
rather spend time with "EverQuest" than with
her. Unfortunately, she's not alone.
The "EverQuest widow" phenomenon has spawned
online support groups like Spouses Against 'EverQuest'
and 'Everquest' Widow(er)s.
Grace Kim and her boyfriend, Steve Chow, are both members
of "EverQuest" Widow(er)s. Chow spent four
or five hours a day playing the game until he realized
it was an addiction.
"It was kind of like smoking, in a way," Chow
said.
"You kind of know you should stop, or maybe that
it's not good for you if you're waking up in the morning
playing this game a couple of hours and then going to
work," he said.
Chow eventually quit altogether, although now he does
play some PlayStation 2 games on a regular basis.
Psychologists say obsessive gaming is a symptom of bigger
problems. Sherman says you must look at other things
to identify the root of the gamer's addiction.
"The more a person is feeling good and secure and
happy and positive with their partners, they don't have
this need, this urge to withdraw and escape," he
said.
Barnes agrees. An avid gamer herself, she says "EverQuest"
was only making existing problems in her marriage worse.
"I would tell the widow it's not 'EverQuest,'"
she said. "It's something else in the relationship
that's not working."
Posted February 10, 2003
TV

October 19, 2000
"What Does Your Online Behavior Mean?"
By Michael Singer
On your average day, 46 million Americans surf the Internet.
Does your online behavior reflect how you act offline?
Digital West, a production of San Francisco's PBS affiliate
KQED-TV, will ask a clinical psychologist, researcher
and online community expert what our online activity
reveal about our personalities and identities.
Lee Rainie, Director of the Pew Internet & American
Life Project, whose organization contributed to the
report says their research is based on an eight-month
random phone survey of 13,000 adults in the U.S.
"From the survey we were able to find out that
51 percent of Americans have computers in the home and
that about 40 percent of those people are online."
Rounding out the discussion will be Online Community
Strategist, Dr. Amy Jo Kim and Dr. Richard Sherman a
clinical psychologist.
|
|
|
[top]

ONLINE
(Partial list)

Email Virus Hits Major US firms | Go
To Article
Facing Down the Downturn | Go
To Article

Keeping Kids Safe on the Internet: Parent Power!
| Go
To Article

A Call For Help:
Employee-assistance programs flourish in tough times
| Go
To Article

Mentors of the Mind
Men who wouldn't go anywhere near traditional therapy
seem more willing
to accept short-term career and personal guidance from
'coaches'. | Go
To Article

The Independent Practitioner
A Funny Thing Happened on the Way to Summer Vacation.
| Go
To Article
IN-PRINT
BRIEFINGS
Psychologist Beware—Managed Care Revisited
Summer 2004 | Go To Article
“Law and Order” and September
11th
January 2002 | Go To Article
When is it All Right to Say No
July/August 2004 | Go To Article
“Original ideas:
Internet 0
Humanity 1,000,000,000,000,000”
November/ December 2000 | Go
To Article
TALK TO AN EXPERT, FOR $19.95
Sept./Oct. 2000 | Go To Article
A Special Thing Happened on the Way to Writing this Article
September/October 2007 | Go
To Article
Confessions of a Recovering Managed Care Provider
March/April 2005 | Go
To Article
Alice in HIPAA Land
July/August 2003 | Go
To Article
Reality TV and the New Breed of Patient
May/June 2003 | Go To Article
Meeting with Vice President Al Gore
December 2000 | Go
To Article
[top]
::articles
Kournikova’s Love
Latest Virus Hits Dozens of Firms
By Sascha Segan
Feb. 12, 2001
Why Anna Kournikova?
Like the ninth-ranked female tennis star herself, the
virus using her name is more provocative than destructive.
Using the tennis star who turns more heads with her
physique than her backhand is a blatant attempt to appeal
to libido, according to psychologists and virus chasers
alike. With her name attached to a JPEG file, it is
no wonder the virus spread so quickly, according to
virus experts.
Kounikova, who has never won a major tennis tournament,
just surpassed hunky basketball star Michael Jordan
as the most downloaded athlete on the Web.
"She's a very popular athlete who has never won
a major tournament but all her matches are watched and
very popular," said James Thomas of Trend Micro.
"She is beautiful."
One psychologist speculated that an obsessed fan may
be the culprit.
"If you attach a provocative name or words to an
e-mail, the perpetrator thinks people will be more likely
to open it," said Richard Sherman, a Los Angeles-based
psychologist.
But who would do such a thing?
"It's the idea of the crazed and obsessed fan,"
said Sherman. "When someone is obsessed they feel
a kind of unrequited love that they want to broadcast."
Like the ILOVEYOU virus, Sherman said the opportunity
to receive a photo of the tennis star was as enticing
as receiving love last year. What better time to get
a JPEG of a pretty, young tennis star than around Valentine's
Day?
In fact, the 18 to 35-year-old male group is very much
aware of the tennis star with the great legs, said Robert
Hermeryck of Trend Micro.
"She is gorgeous" said Hermeryck of antiviral
firm Trend Micro. "She's beautiful. Men and women
alike want to look at her."
Viruses spread by provoking their targets, according
to Sherman. Sometimes out of a feeling of powerlessness,
virus creators use words that may scare potential victims.
Sometimes, out of obsession they use a celebrity name.
"They are trying to connect to people in one way
or another," he said. "With the ILOVEYOU,
it was a sick trick as a way to seduce people. With
Anna Kournikova it is a kind of admission of their love,
unrequited. But with people who have personality disorders
it could be a multitude of reasons."
— Rose Palazzolo
[top]
Facing Down the Downturn
The R-Word Can Terrify, But Psychologists Say People
Are Resilient
By Robin Eisner
N E W Y O R K, Jan. 11, 2001 — With a son in law
school and a daughter in college, 54-year-old Frank
Stevens, believes his professional life is about to
unravel.
Stevens, a salesman in the high-tech sector, senses
that the consulting company he works for is going to
shut down, unable to compete in the tightening economy.
Although the 6-month-old Southern California firm is
a subsidiary of a major company in the Midwest, Stevens
— who asked that his real name not be used —
says the start-up satellite business doesn't have the
marketing or advertising dollars from the company necessary
to grow.
"They don't have money," says Stevens, who
sells the company's computer networking services. "They
are cutting back."
He took the job, after 20 years at another major corporation,
because of the high salary and the bracing challenge.
Now, he has withdrawn $40,000 from his seven-figure
savings, because the sales commissions he depended on
have dried up. He is selling real estate to pay off
debt. And he's looking for a new job.
Changing Times
One day it's Sears, Roebuck & Co. cutting thousands
of jobs. Then, it's Rupert Murdoch "consolidating"
the Fox News online division, where hundreds were handed
pink slips. After almost a decade of growth, an economic
slowdown appears to be coming to both traditional and
new-economy businesses in the United States. Although
the unemployment figures are still very low, there's
instability, signs of possible turmoil and worry.
Most Americans don't save money, let alone prepare for
financial doldrums. But soon they may have to adjust
to a shrinking economy with fewer jobs and less disposable
income. For some people it will be déjà
vu all over again, reliving the 1982 and 1991 downturns,
which eventually reversed. For younger workers used
to moving around freely, it may be their first experience
of shrinking opportunity.
While such conditions could initially discourage and
depress people, psychologists with expertise in financial
issues say it's not all doom and gloom: Business cycles
are inevitable, and dips help society return to core
values of family, friends and community. Eventually,
philanthropy, banding together and frugality become
fashionable in lean times, as consumerism was trendy
in booms.
Economists tell us the economy is slowing down, but
not quite as badly as prior downturns of the past two
decades, when growth lingered at 1.5 percent. The Commerce
Department, in its latest figures, reports the third
quarter U.S. gross domestic product last year was only
2.2 percent. That's down sharply from a 5.6 percent
rate set in the second quarter, and is the slowest growth
in four years.
Still, don't start using the R-word — we're not
experiencing a recession, which is defined as two consecutive
quarters with negative economic growth.
Setting Priorities
At times like these, psychologists say the most important
thing is not to panic. People need to take a realistic
look at their finances and consider the worst.
"When money starts getting tighter, people have
to start looking at their budgets and determine what
they can do without," says Maurice Elvekrog, a
psychologist and chartered financial analyst from Bloomfield
Hills, Mich. "Parents should talk to their children
about economizing, explaining that they may have to
do without some things but that the family will remain
together and manage."
Back in California, Stevens forewarned his children
during Christmas about his situation. "I spoke
to them honestly," he says. "They are old
enough not to have to be shielded from life." Tuition
for the kids will still be met, but gift giving will
be curtailed, Stevens told the family in a pre-Christmas
gathering.
Americans may also need to reconsider what is important
to them, that having the latest consumer gadget may
not be so significant. "People may have to shop
differently and try to find value in relationships and
personal activities that do not cost anything,"
says Richard Sherman, a clinical psychologist in Tarzana,
Calif. who works with large companies advising them
on downsizing.
People may want to consider a downturn an opportunity
to make a career change. Stevens says he is considering
living on his retirement money and settling for less
income in another profession. "I always wanted
to be a teacher," he says.
The Meaning of Money
Psychologists acknowledge that loss of money can be
difficult because our society associates love, power
and freedom with money. And since people define themselves
so much by their jobs, a job loss — or even the
fear of losing one's job — can threaten their
very sense of identity and self-worth.
James Gottfursht, a psychologist specializing in money
and employment issues from Los Angeles, suggests people
take small steps to adjust to changing times, cutting
back, say, on the number of videos they rent a week
or the number of times they eat dinner out. "Smaller
losses are easier to face," Gottfursht says.
As people have less, thriftiness will become "chic,"
as it has in past times, Gottfursht says. "Instead
of conversations about spending, discussions might veer
towards spending less money on dinners or vacations,"
he says. "Once people break free of the addiction
to money, they realize that they really didn't need
it so much."
Facing Loss
If you hit a crisis, like losing your job, you will
be grateful for re-cultivating your friends and family,
who can help you through it. "The worst thing you
can do is isolate yourself," says Sherman. "Exercise
and eating right is as important now so you don't get
depressed."
Keeping perspective also is key. "You may have
lost a job, you didn't lose an arm," says Neil
Lewis, a psychologist in Marietta, Ga., who advises
companies about downsizing.
Lewis advises the recently unemployed to "take
stock, take charge and take action": First, look
at cash flow. Then, take responsibility, and don't blame
others (or yourself) for your situation.
"Instead, they should take action and make looking
for a new job, a full-time job," Lewis says. People
should talk to friends and associates, and join support
groups to talk to others who may be going through the
same thing.
Human beings have amazing recuperative powers, and will
manage, says Lewis. "Unfortunately, life sometimes
is not easy," he adds.
The Survivors
The person who receives a pink slip, however, is not
the only one who suffers, the experts say. If a company
keeps cutting its staff, those who remain often pick
up the additional work to a point of what can be diminishing
returns, says Mitchell Marks, a psychologist who specializes
in businesses from San Francisco.
"People may be willing to run the treadmill and
work hard if there are bonuses and rewards at the end,"
Marks says. "But for fewer benefits, people may
decide to slow down."
With a possibility of increased unemployment, it also
becomes difficult for people to find new jobs, should
they want to jump ship. Young people used to ever expanding
prospects may get resentful.
Managers will have to find ways to motivate remaining
employees to increase output if raises and other perks
become less likely. "Managers should be proactive
and communicate with employees that they may have to
work harder now with the hope that prosperity will return
and so they do not lose their job," Gottfursht
says.
Should sluggishness continue, though, the have-nots
may start getting angrier with the haves. "There
is a growing divide among the rich and poor," Marks
says. "When things are rosier, Middle America didn't
begrudge the haves. But in a tightened economy, the
middle class may not be able to tolerate the high salaries
of CEOs and athletes."
Frank Stevens takes antidepressants and sees a psychologist
to help him cope. He is optimistic he will find another
job, after being to three job interviews recently. "I
am a salesman," Stevens says. "I am not afraid
to sell myself about how good a worker I have been …
If I could do it for someone else, I could do it for
a new employer."
[top]
Keeping Kids Safe on the Internet: Parent Power!
By Natalie Walker Whitlock and Marilyn Martinez
Now for the good news: Parents have more choices and
tools than ever before to help keep their families safe
online. They can stock a technology toolbox, full of
filtering, blocking, monitoring and tracking software.
They can use the parental controls included with their
ISP or online service and can use only kid-friendly
search engines and portals to limit children’s
exposure to inappropriate sites.
“I’m all in favor of a kid’s invasion
of privacy because of the danger potential here,”
says child development professor Polland. “You
cannot take the chance. Because kids feel so safe and
so bright and so confident about how to beat the system,
they are in danger.”
Some parents share an online account and password with
their child to keep tabs on their children’s e-mails
with online friends. Parents can even track chats and
instant messages in real time, even when they are away
from home. There are also non-tech options such as creating
a Family Internet Use Contract (www.safekids.com/contract.htm
) Which options you use depends on your child and your
own parenting style.
But while technology has provided parents with numerous
options, high-tech safety tools should be only a piece
of the solution – not the whole pie. Indeed, experts
repeatedly caution against relying solely on high-tech
babysitters to keep kids safe online. “Technology
is not a replacement for good parenting,” says
America Online chairman Steve Case.
O’Connell-Jay, who now educates parents, teachers
and police on the subject of Internet safety, recommends
that parents get involved in their children’s
Internet life – even ask their kids for lessons
if they’re computer illiterate. In her sister’s
case, “Nobody knew, because nobody was computer
literate,” she says.
The key to keeping kids safe on the Internet today is
parents who recognize the possible dangers, understand
the technology, and take the time to be involved in
their child’s online activities.
“Parents who understand the Internet and monitor
the time that a child spends online offer the best protection,”
says Richard Sherman, Ph.D, a psychologist specializing
in children and Internet issues. “Kids need appropriate
monitoring by parents at home to prevent inappropriate
behavior online."
Natalie Walker Whitlock is the author of A Parent’s
Guide to the Internet (Parent’s Guide Press, 2003).
Marilyn Martinez is the associate editor of L.A. Parent
magazine, a United Parenting Publication.
[top]
VITAL SIGNS
A call for help
Employee-assistance programs flourish in tough times
By Kristen Gerencher, CBS.MarketWatch.com
Last Update: 12:02 AM ET March 27, 2003
SAN FRANCISCO (CBS.MW) - After a long, frustrating search
for a psychotherapist in her health plan, Laura Walker
found an available counselor through an unlikely source
- her mother's employee-assistance program.
Because the EAP covered immediate family members, Walker
achieved through a single phone call what two-weeks
of cold calls failed to produce: A list of doctors taking
new patients who would accept her health insurance.
"I felt like the situation was hopeless,"
says Walker, 25, upon being turned away by numerous
therapists. After answering a few questions to assess
her need and preferences, the EAP found a match within
a day or two. "It got me an appointment I wasn't
able to get myself."
Once known as a first stop for treating workers' drug
and alcohol abuse, EAPs now provide a host of resource
and referral services to people who otherwise would
take care of their sundry problems on the boss' watch.
And unlike a health plan, many EAPs offer counseling
sessions for free, with no co-pay or deductible acting
as a disincentive.
The programs can provide a one-stop shop or neutral
third-party analysis to workers in distress, whether
they're dealing with divorce, a troubled teenager, ballooning
debt or an elderly relative's decline.
Most people self-refer to the programs, which often
function as "derailment prevention" for employees
slipping at work, says Richard Sherman, a clinical psychologist
and EAP consultant in Tarzana, Calif.
"It helps keep good employees functioning well
on the job," Sherman says. Employers "want
to prevent the employee from going off the positive
course for the benefit of the company."
Guarding productivity
Despite widespread belt-tightening, employers aren't
doing away with the benefit, analysts say.
In fact, as the economic slump drags on and the war
with Iraq heightens anxieties, EAPs appear to be living
up to their promise of keeping workers productive and
providing them with alternative solutions to problems
that distract them.
In 2002, 71 percent of large employers offered an EAP,
up from 64 percent in 1998, according to Mercer Human
Resource Consulting. Last year, 14 percent of small
employers with 10 to 499 employees extended the benefit,
up from 12 percent five years ago.
The vast majority of companies offer screening and referral
with short-term counseling, with screening and referral-only
programs the next most popular choice. The remaining
employers opt for a phone-based program.
EAPs often complement health plans and are "something
employers are really striving to maintain and promote,"
says Kate Sullivan, health-care policy director at the
U.S. Chamber of Commerce. "They're almost always
offered separately and apart from the health plan so
employees not involved in the health plan can have access."
Many companies placed a "a renewed sense of importance"
on EAPs after September 11, says Richard Chaifetz, chief
executive of ComPsych, a Chicago-based consulting firm
and EAP provider that covers 7 million Americans. Calls
for help jumped 15 percent last week when the war with
Iraq began, but have since leveled off.
"There's a huge return on investment in terms of
productivity, performance and absenteeism," Chaifetz
says. "The amount of money employers pay to get
an EAP typically returns three to five to 10 times as
much in terms of measured savings in the first year."
User-friendly coverage
Employers contract for different packages, with most
opting for a plan covering mental health, legal and
financial services and work/life services such as child
and elder care, Chaifetz says. Some programs provide
unlimited financial and legal counseling.
Typically, help is available at any time, seven days
a week and begins either online or with an 800 number,
he says. About 4 to 6 percent of eligible employees
take advantage of their EAPs on average, and most seek
help with relationship and family issues.
What's more, the programs often allow a certain number
of visits per incident as opposed to limiting access
more generally, Chaifetz says.
"If someone calls in for a divorce issue and three
months later calls in for a child who's not doing well
in school, that would start the clock again."
Confidentiality and mental health
Though companies generally strive to get 5 to 10 percent
of their workers to use their EAP, many employees are
afraid to make contact because of confidentiality concerns,
says Tom Billet, a senior consultant at Watson Wyatt.
But EAP providers only report the number of employees
who use the service back to the employer and not names
or details, he says.
"You call the EAP provider and no one at the company
ever knows you call," Billet says. "Confidentiality
is what they live and die by. If it at all came out
that they were releasing names to employers, they'd
be out of business pretty quickly."
EAPs, which have seen rising education levels among
their providers over the years, are particularly useful
for those seeking mental health advice, Sherman says.
"It sometimes takes the stigma away that some people
have toward going for psychological help," he says.
Unlike other types of health care, most people don't
have a long-standing counselor in their portfolio of
doctors and may feel embarrassed or overwhelmed when
searching for one, Billet says.
[top]
Monday, June 18, 2001 | LOS ANGELES TIMES
Mentors of the Mind
Men who wouldn't go anywhere near traditional therapy
seem more willing to accept short-term career and personal
guidance from 'coaches.'
By BENEDICT CAREY, Times Health Writer
You don't have to get in touch with your feelings: You
can manage them. And instead of plunging into self-analysis,
you can concentrate on innocent-sounding things such
as emotional intelligence, better relationship-management
skills and a more successful personal style.
What regular guy would consult a therapist when he can
have . . . a coach?
Though most men are still very reluctant to seek traditional,
one-on-one therapy, more and more of them are now consulting
professionals who call themselves life or career coaches,
psychologists say. Coaching is not the same thing as
therapy, experts agree. One is an open-ended exploration
of the origins of emotional makeup; the other is usually
short-term and focused on achieving concrete goals,
often in the context of career.
But the number of experienced therapists who now consult
as coaches has at least doubled in recent years, psychologists
estimate, and they are exposing more men than ever to
the benefits of psychological self-evaluation.
"The very word 'coaching' is appealing to people,
especially men, and allows them to access basic psychological
principles in a way that's socially acceptable,"
says psychologist Bertram Edelstein, who runs an executive
coaching practice, the Edelstein Group, in La Jolla.
"You begin talking about work, and that's the one
place where most men feel competent, or at least comfortable,"
says Richard Sherman, a psychologist in Tarzana who
does coaching and runs his own clinical practice. "And
at some point you begin to ask about work-life balance,
and that acts as a bridge into the personal life."
Steve Finden, a 36-year-old insurance company executive
living in Encinitas, began consulting with Edelstein
about three years ago as part of a company-sponsored
effort to improve teamwork. Finden describes himself
back then as "a typical guy, pretty wrapped up
in myself, and in my work," and hardly the type
to seek individual psychotherapy.
After taking a personality test and reviewing reports
of how others perceived him, Finden got a lesson in
self-awareness, he says. "I thought I was an effective
strategic thinker, a good communicator," he says.
"It turned out I was about the only one who thought
so."
Part of the problem was that others didn't think that
Finden passionately believed in what he was saying.
That apparently superficial observation got him thinking
more deeply about what shaped his personality. "You
can't help but think about where your habits and style
come from, how you got that way, and how you come across
at home," he says.
Often enough, Edelstein says, people trace their personal
style at work back to their family of origin, and sometimes
even back to some defining crisis, such as losing a
parent, the illness of a sibling or an alcoholic parent.
And when it's effective, says Edelstein, career or life
coaching induces changes that usually move from the
person's work life into their private life. "Nine
times out of 10 times I hear from the spouse that the
side effect from coaching is improved personal relations
at home," he says. Men in particular are more likely
to respond to advice when it concerns their effectiveness
or promotability. "Their spouse could have been
saying the same thing for years and they ignored it,"
he says.
"We weren't having problems to start with,"
says Finden's wife, Elizabeth, "but I would say
that now that he's managing people and he's learning
to work with them, he's become more present, a better
listener, less concentrated on himself."
* * *
Analysts attribute therapists' move into coaching to
two phenomena: managed care, which has put a squeeze
on longer-term psychotherapy; and the growth of Internet
and tech companies in the 1990s, which happened so quickly
that employees and managers had to learn social and
management skills on the fly. "These are the IT
types who are accustomed to working by themselves, alone
in a room, and suddenly they're managing 500 people
and they know nothing about human dynamics," says
Steven Berglas, a psychologist and author who has an
executive consulting practice in Marina del Rey.
The technology itself has changed the way people relate
to one another, Sherman says. "I'm now dealing
with employees with virtual offices seven days a week--cell
phones, faxes, computers, Palm Pilots--and part of what
I try to do is help them not lose sight of their other
life, their family and friends."
And by and large, these are not men who seek solutions
on the couch, despite the popularity of shows such as
"The Sopranos," in which mob guy Tony Soprano
regularly confers with a therapist. Overall, men account
for only about a third of all people seeking some kind
of individual psychological attention, psychologists
say, which is not much different from a decade ago.
"The problem is that therapy itself is antithetical
to everything it is to be a male in this society,"
says Rob Pasick, a psychologist who teaches in the business
school at the University of Michigan. He co-edited a
1990 book called "Men in Therapy" that helped
fuel a surge of interest in men's issues. "Asking
for help, showing weakness, admitting you have no control,
revealing yourself to a stranger--these just aren't
things guys are taught how to do."
So it is that therapists-as-coaches are now resolving
personality problems--of ego, temper, anxiety, fear
of failure--for people they otherwise would never see,
most of them male. If Tony Soprano is altering the perception
of psychological help in the popular culture, they say,
then life and career counseling is doing the same in
practice, in men's work and home lives.
Glenn Good, a psychologist at the University of Missouri
who has written a guide to counseling males, says the
growth in coaching represents a broader trend that is
bringing psychological services to men in more accessible
ways. "We've learned, for example, that traditional
men's men will talk about their personal lives, but
they're more likely to do so in a seminar, or in a career
context" than a traditional psychotherapy setting.
* * *
For all that, psychotherapists still have some strong
reservations about life or career coaching. For one
thing, the field has no widely accepted professional
standards; the International Coach Federation, a professional
organization in Washington, D.C., estimates that there
are more than 10,000 people calling themselves coaches,
and only about 600 of those have completed the Federation's
certification process. The Federation's Web site (http://www.coachfederation.org/)
allows individuals or companies to search for certified
coaches in their area.
Another risk is overtreatment--therapists luring clients
into longer-term psychotherapy who may not need it or
want it. "In coaching, the biggest danger is that
you don't let go when the behavior you're hired to treat
goes away," says Berglas. "Once the problem
is solved, your job is done; that's it."
Finally, life or career coaching can never be a substitute
for psychotherapy. There are many men whose problems
go deeper than any occupational personality test, and
trying to "coach" them through it is irresponsible,
psychologists say.
Craig Paxton, a 34-year-old Web designer living near
Ann Arbor, Mich., ended up in Pasick's care after a
job ended badly. He was losing his faith that he'd ever
find work again. "Confidence was becoming a huge
problem," Paxton says. "It didn't matter how
much people would tell me how good a job I was doing;
I still saw the flaws."
But further discussion revealed that Paxton's anxieties
ran deeper, and were partly related to the suicide of
a good friend. He showed signs of depression as well.
Paxton was referred to regular therapy and now attends
a men's therapy group. "I just don't understand
the stigma that therapy has for men anymore," he
says. "You've got to support the world on your
shoulders, and you can't ask for help? If I can do it,
anybody can."
Psychologists say that, whatever its limits, the arrival
of psychology in the context of life and career goals
has at least tipped off many men to what therapy can
offer. Says Finden, "I've figured out about as
much as I want to know at this point, and I think it's
had a nice spillover effect on my personal life. You'd
need to go much deeper to understand everything. But
at least I know it's there."
Copyright © 2001 Los Angeles Times
For information about reprinting this article, go to
http://www.lats.com/rights/register.htm
[top]
The Independent Practitioner
APA Division 42, Fall 2000
A Not So Funny Thing Happened to Me on the Way
to Summer Vacation
(The following is a true account of one psychologist’s
recent, somewhat alarming experience with a major managed
care company. Only the names have been changed.)
As I anticipated writing an article for the summer edition
of The Los Angeles Psychologist, I thought that this
would finally be the time where I could collect my thoughts
and write a somewhat lighthearted piece in keeping with
our childhood recollections regarding this time of the
year. That was until Dr. R. recounted to me his hair-raising
encounter with a large mental health managed care company.
I thought that his story was so important to many of
us in our profession that it was worth retelling in
its entirety.
Dr. R. is a psychologist who has been in clinical practice
for over twenty years. He has a successful practice,
which includes both managed care and fee for service
patients. He also does some consulting. In addition,
he has been an active member of a number of professional
organizations and has assumed various leadership positions.
Further, over the years he has served as an oral examiner
for the licensing of new California psychologists and
has been a provider member from the community on a number
of credentialing/peer review/quality improvement committees
for different managed care companies. In addition, through
Continuing Education programs, readings and consultations,
he has worked hard to keep up with changes in the law,
ethics, record keeping, and community standards as they
relate to the practice of psychology. Dr. R. typifies
the many well trained, quality psychologists that make
up our profession at both the state and local levels.
This is why Dr. R. was quite surprised and alarmed when
he recently received an overnight letter from the Director
of Provider Operations for a large managed care company,
one for which Dr. R. has always served in good standing
since joining that panel in 1989. The letter in part
stated that, while this particular organization had
appreciated his participation in its panel, “after
careful review” the Credentialing Committee had
decided to terminate his membership in the network “due
to a low client satisfaction rating.” Termination
was to occur 90 days from the date of the letter. This
would allow the provider to complete the treatment of
“covered members” or to “contact a
case manager…to discuss transition options.”
Further Dr. R. was entitled to a “one-time”
review of the decision by a medical director as long
as this review was requested within 30 days of receipt
of the letter.
Dr. R. described his panic as he read the letter. At
one point, patients from that managed care company had
made up more than 20% of his practice. He knew of no
ethical code violations in his practice of psychology.
This particular managed care company periodically would
send profiles of a provider’s performance. Dr.
R did remember that when he attended one of this company’s
recent training programs, the presenter had indicated
that very few patients ever respond to patient satisfaction
surveys. Nonetheless, his scores had always been in
the acceptable range, including the most recent one
dated December 1998. In fact, the scheduling time between
a patient’s first call to his office and an initial
appointment averaged only 5 days while that company’s
standard for non-urgent sessions had been 14 days. Further,
Dr. R. recalled easily passing a site visit which this
company had conducted in the summer of 1999.
Immediately, Dr. R. called the person whose name was
on the letter. To his dismay, the assistant told him
that the Director of Provider Operations was out of
town for the next two weeks. The assistant went on to
tell Dr. R. “that’s okay because this will
give you more time to prepare your defense.” Dr.
R. was incredulous and questioned, “What defense?
I don’t know what if anything I did wrong given
that there was no supporting documentation in the termination
letter.” The assistant responded, “We’re
sorry but we don’t have that information here.”
Dr. R. quickly realized that he was talking to someone
who, while she may have been well intentioned, was merely
a clerk who had no power whatsoever in this matter.
Despite several calls to that office, she was unable
to give Dr. R. the name of anyone who might be in authority
to shed any light on this matter.
According to Dr. R. the situation went from bad to worse.
He had previously liked being a member of that panel
for several reasons including that from time to time
many of his old patients would request to see him again,
even four or five years later, as new problems emerged
in their lives. It was only one week later that such
an old patient informed Dr. R. that when she had called
the managed care company to request authorization to
see him, she was told that this was not possible since
he was being removed from the provider panel. No reason
was given to the patient.
At that point, Dr. R. became even more concerned since
he recalled that on many hospital privilege forms and
other organization applications, there is a question
which states, “Have you ever resigned or been
asked to resign from the staff of any hospital or organization
because of problems regarding privileges, credentials,
or unprofessional conduct?” Dr. R wondered whether
being involuntarily removed from a managed care company
would fall into this category and haunt him for years
to come.
Because Dr. R. had had some experience with other managed
care companies and related organizations, he was determined
to assertively follow through, to determine if there
had been a mistake made, or to see if he had inadvertently
done anything wrong to warrant this type of action.
He talked to an attorney from the Legal and Regulatory
Affairs Office of the APA Practice Directorate. She
indicated that most of the contracts between many managed
care companies and psychologists are one sided because
a provider can easily be removed in thirty days “without
cause.” She indicated to Dr. R. that if he were
really serious about pursuing this, he might have to
hire an attorney and incur the necessary expenses.
As the time passed, Dr. R. became even more frustrated
and worried. He still did not know what he supposedly
had done wrong, if anything. In his involvement with
committees from other managed care companies, he knew
that before a provider is ever dropped “with cause”
from those panels, he or she is notified and given great
detail regarding what the problems or issues are and
what corrective measures can be taken. Dismissal from
the provider panel is reserved for the most egregious
infractions. Mentally, Dr. R. kept reviewing a fraction
of the possibly hundreds of cases that he had seen for
this particular company over the years. Nothing even
remotely negative stood out. He even recalled a conversation
that took place a few weeks earlier with a senior psychologist
from this managed care company in which she had been
very positive towards his work as she then referred
him a difficult case.
Given that Dr. R. was getting no response by going through
proper administrative channels, he decided to try to
communicate directly with both the local and national
medical directors of this managed care organization.
He was quite pleased with the reception that he received.
In fact, one of these senior psychiatrists actually
took it upon himself to review the case and be the one
to present the “findings” to the credentialing
committee.
What the medical director found was quite disturbing.
First, he indicated “the manner in which Dr. R.
had been informed without means of redress” had
been wrong at least in his “humble opinion.”
What was equally troubling was that the alleged “complaints”
against Dr. R, for which he almost been cavalierly dropped
from the panel, should not have ever gotten to that
stage in the first place.
What was the nature of the complaints that so jeopardized
Dr. R.’s chances of being retained by this panel?
One must remember that Dr. R. was being considered for
recredentialing in 2000 and had successfully gone through
the credentials committee process every two or three
years since his initial acceptance to that panel. First,
in 1996, a prospective patient had complained that she
had tried unsuccessfully to contact Dr. R. to make a
first appointment and that he had never called her back.
Dr. R. questioned this since he has a secretary and
together they have a good track record of returning
all calls in a timely manner. Dr. R. even wondered if
the patient had actually had the correct phone number,
but four years later and not knowing the name of the
patient, it certainly would be impossible to track this
down. So much for serious complaint number one.
The second complaint was even more illusory and had
nothing to do with actual patient satisfaction but with
treatment planning and recommendations. It was even
more peculiar how this generated any flack whatsoever.
Dr. R. briefly saw a depressed patient in 1993 who,
up until one month prior to the start of treatment,
had been abusing cocaine. Dr. R. recommended to the
patient that he attend frequent 12 step CA meetings
along with individual psychotherapy. In 1996, when the
managed care company had an outside EAP reviewer apparently
look over various clinicians’ treatment plans,
he determined that this patient should have been referred
to either an inpatient drug rehab facility or a structured
outpatient program. The reviewer who did not see Dr.
R.’s records, but only a very brief structured
treatment plan form, could not have had enough information
to disagree with the clinician’s findings. Further,
the medical director agreed fully with Dr. R.’s
recommendations, not the reviewer’s. Parenthetically,
Dr. R. holds an APA Certificate in Proficiency in Alcohol
and Psychoactive Substance Disorders. If anyone at the
managed care company had any concerns about his approach
to treatment, why hadn’t someone ever called him
to discuss this? What is even more troubling was that
this was a case from 1993 being used to affect the provider
status of a psychologist in 2000, seven years later.
Dr. R. waited anxiously until the next credentials committee
meeting. Finally, he received word from the corporate
medical director, who informed him that the committee
had voted to retain him on the provider panel and to
immediately lift the suspension on referrals. This suspension
should never have occurred in the first place. He also
indicated that the medical director who had presented
the review had advocated “energetically”
for Dr. R.
What can we learn from Dr. R.’s experience?
First, it is important to recognize that the managed
care companies do have on their staff some decent and
wonderful professionals, including psychologists and
psychiatrists, who believe in the quality of patient
care, are psychologist friendly, and want providers
to be treated fairly. However, we also must remember
that huge consolidated corporations are currently controlling
the mental health coverage of millions of patients.
Further, important administrative decisions may sometimes
be made almost independently of the clinical staff that
they have employed. There has to be something seriously
wrong for a company to even consider the removal of
providers for essentially no valid reasons. One can
only speculate on the possible rationale for such a
decision—the wish to decrease the size of the
network or the desire to eliminate those psychologists
who under older contracts may be receiving a slightly
higher reimbursement rate than newer providers. Dr.
R. has had years of experience in working with insurance
companies and as a result, was able to mobilize a concerted
effort to retain his provider status. My concern is
for those psychologists who may be excellent clinicians
but less familiar with the system. I will leave to the
readers of this column to draw your own conclusions.
Given this, it is incumbent upon psychologists to interact
with these companies from both a good professional and
business sense. For instance, one should consider periodically
checking on the existence of any possible patient complaints
just as, in our personal lives, we may need to check
periodically on the status of our credit rating. The
time to do this is not when one is about to be recredentialled.
One may also want to consider having an attorney review
new contracts with such companies, in advance of resigning.
And of course, it is important as psychologists that
we diversify so that we are not beholden to any one
managed care company. Further, the more one can expand
our professional psychologist repertoire and become
more expert in specialized areas, we will be successful
independent of any organization.
By the way, some of you may be wondering how I knew
so many of the details of Dr. R.’s struggle with
that particular managed care company. That is because
I actually am Dr. R. Now, I can go back and enjoy the
rest of the season. I wish all of you and your families
a pleasant, restful, and energy reviving summer.
Richard Sherman, Ph.D., is a psychologist
in private practice in Tarzana, California. Dr. Sherman
is the 2000 President of the Los Angeles County Psychological
Association.
This article originally appeared in the July/August
issue of The Los Angeles Psychologist and is being reprinted
with permission.
[top]
BRIEFINGS
Summer 2004
Psychologist Beware—Managed Care Revisited
I recently got a call from a large Managed Care company.
“We want you to do an evaluation of one of our
subscribers and we need this done right away,”
the woman on the line stated. “We will give you
up to three visits to do this.” She went on to
state, “If you then want to see this patient for
therapy, you just have to fill out the Outpatient Treatment
Report. She indicated that the prospective patient had
just been released from a short stint in jail and was
having work and family problems. When I asked for more
clarification such as why she had been incarcerated,
given that I did not want someone who might have recently
been violent coming to my office, without at least a
little warning, she indicated that she could not disclose
this information. When I asked how much I would be reimbursed
for this evaluation, she curtly replied, “It’s
in your contract.”
This call came at the right time because it gave me
more reasons for resigning from most if not all of the
managed care company panels. Like several of my colleagues,
I had agreed to join these panels several years ago
for a variety of reasons: (1) managed care was literally
taking over Southern California with the perceived result
that if one did not sign up, one might not have access
to most patients, (2) by agreeing, along with many other
psychologists, to participate and see patients for a
discounted fee, hard working employees and their families
would be able to get first-rate mental health care for,
at most, a nominal co-pay, and (3) we were told that
the managed care companies would pay in a timely manner
with no bureaucratic red tape. How wrong these assumptions
have proven to be. One point however does still hold
some weight. I have several patients that I have seen
off and on for an extended period. If I were to completely
stop seeing them through their managed care plans, some
would not be able to stay in treatment even at a reduced
fee. Unfortunately, managed care continues to have a
negative influence on the practice of psychotherapy,
including some loss of control over clinical decisions,
inappropriate or insufficient treatment allowed, additional,
often needless paperwork, and a decline in revenue due
to low reimbursement. Reimbursement rates do not take
into account inflation with several plans holding fees
at 1987 rates. According to the Bureau of Labor Statistics
and taking into account inflation, a fee of $70 then
is equivalent to $114.74 today—thus a net loss
of almost $45 per hour for the psychologist. At the
same time, the CEO’s of the largest healthcare
insurance companies are making millions of dollars per
year.
According to Yahoo Finance, for the fiscal year 2002
(including salary and bonuses), William McGuire, M.D.,
the Chairman and CEO of United Healthcare earned $9.4
million while Mr. Howard Phanstiel, Chairman, President
and CEO of PacifiCare earned $3 million.
Whatever the managed care hourly rate that the psychologist
earns is also somewhat deceptive given the additional
minutes to hours that one has to spend related to the
managed care created bureaucracy. A typical scenario
of additional time that the psychologist (and/or support
person) must spend is as follows:
Before the patient’s first visit:
• Call insurance company for authorization and
verify mental health outpatient benefits (up to 15 minutes)
• Obtain the different reimbursement/co-pay schedules
depending on whether the diagnosis will be parity or
non-parity
• Assemble new patient information with forms
specific for the individual insurance company (5 minutes)
After the patient’s visit:
• Document specific information that the insurance
company is requesting which may be more in depth than
is needed to effectively treat the patient (10 minutes)
Requesting additional visits:
• Prepare treatment plan (can be as brief as a
couple of minutes or, if a detailed report is needed,
as long as 30 minutes or more, depending on the insurance
company)
• Talk to a care manager regarding the patient’s
progress
(5 -15 minutes)
Billing and other administrative issues:
• Contact insurance company if payment has not
been received in a timely manner (10-15 minutes)
• Analyze Explanation of Benefits to make sure
that payment is correct (up to 5 minutes)
• If EOB is not correct, psychologist must spend
time with insurance company to rectify any errors (15
minutes or more)
• Explain to the insurance company the difference
between parity and non parity benefits and different
payment schedules (5 -10 minutes)
While the psychologist is getting paid for a 45-50 minute
session, at times, this clinician could actually spend
approximately an additional 75 minutes or more of time
that is not reimbursed. Further, this does not take
into account the amount of time that the psychologist
is placed on hold “for the next available representative”.
This also does not consider the time that the psychologist
has to spend if there is a random chart audit and all
progress notes have to be photocopied and sent to the
managed care company at the psychologist’s expense.
What then is a psychologist to do? New psychologists
are especially tempted to join managed care panels as
a way to more quickly build up a private practice. Other
psychologists who have been on these panels for an extended
period are often torn given that several of their patients
are seemingly locked into the managed care system. Given
the time spent, as outlined above, servicing the accounts
of each patient along with the restrictions that most
managed care companies place on the treatment of those
patients, psychologists could better utilize time in
professional networking and in gaining additional specialty
training which should translate into increased referrals.
Further, we need to support the advocacy efforts of
our professional organizations at the local, state,
and national levels.
Oh, you might wonder whatever happened to the woman
from jail. I reluctantly agreed to see her for a one
time evaluation but …….she never showed
up for the appointment. I wonder if I can charge the
managed care company for the No Show. I doubt it!
[top]
BRIEFINGS
January 2002
“Law and Order” and September 11th
Prior to the September 11th attacks, in addition to
listening to the news during the day, I used to watch
the 11o’clock news—a wrap up of the day’s
events before bed. Every night for the last several
weeks, I find myself watching instead reruns of the
crime program “Law and Order”. While the
show may be somewhat formula-like in style and concept,
I am intrigued by each episode nonetheless. More about
my changed TV watching habits later.
On the morning of September 11th, 2001, I was in Washington,
D.C. as part of a small group of Southern Californians
who are members of a national political organization.
We were in Washington for five days to meet with different
representatives of the federal government. That Monday,
the day before, we had a meeting with Attorney General
Ashcroft. We also met with Deputy Defense Secretary
Paul Wolfowitz at the Pentagon. Ironically, less than
twenty-fours hours before the attacks, we had even had
a working lunch with two noted anti-terrorist experts
who complained that our government was not doing enough
to protect the country from possible terrorist assaults.
The organizer of the conference, as a way to encourage
participation, kept talking in advance that this was
going to be an unforgettable trip. He was so right for
what obviously became the wrong reasons.
That Tuesday morning in Washington was absolutely a
glorious day –sunny, clear, and cool. One of those
picture post card days. Our first stop was the Capitol.
We had heard on the way over that there had been an
accident at the World Trade Center and a vague account
that a plane had struck one of the towers. We had some
concern but most of us visualized a small plane accident,
nothing more. We proceeded into the Capitol rotunda,
greeted by an aide. We were to meet with a House member
who was going to talk with us and give us a tour of
the Capitol Dome. Just then a guard, without giving
a reason, yelled, “Hurry, hurry, everybody get
out now!”
We all ran out as quickly as possible and found ourselves
on the lawn in front of the Capitol, across the street
from the Supreme Court Building, where I saw a U.S.
sharpshooter on the roof. Everyone was pouring out of
nearby buildings. As we saw smoke billowing out of what
turned out to be the Pentagon, we started figuring out
what was going on. We also learned that our hotel had
also been evacuated. While most people in D.C. and those
visiting have cell phones, few were working. We tried
to no avail, to get a hold of loved ones to let them
know that we were all physically fine, but a little
shaky.
That afternoon we were supposed to have visited with
Supreme Court Chief Justice William Reinquist. Instead,
we were on a bus out to “no where” and finally
three hours later ended up in Maryland. (Ironically,
when we returned to D.C. later that day, the same ride
only took approximately 25 minutes.)
Many of us that day experienced the mixed feelings of
shock, sadness, confusion, and even some denial. We
later heard about the plane that had crash-landed in
Pennsylvania. Reports indicated that this particular
plane might have been heading either for the White House
or for the Capitol, if it were not for the heroism of
some of the passengers on board. We possibly owed them
for our safety—they were heroes; we were just
lucky.
Our conference was understandably halted and because
there was a moratorium on all flights from D.C. area
airports, we were essentially stuck in Washington, D.C.,
for three additional days. There was quite a somber
tone as we walked around such places as Georgetown and
saw military police with rifles standing up against
humvee vehicles. The city was on heightened alert yet
initially President Bush wanted all activities to resume
as much as possible. Partly to support this effort and
to show a token defiance regarding the attacks, I even
walked over to the Old Executive Office Building and
took what may have been the last tour of the White House
for some time to come. (Possibly in retrospect, these
activities might not have been the wisest).
Needless to say, each one of us wanted to get back to
California as quickly as possible. I had hardly known
most of the other conference participants; it was interesting
to see how each handled this emergency situation. Several
parents of young children, as one could easily appreciate,
were panicked because they were so far a way from their
families. One recently married young man literally “felt
trapped” being away from his new wife such that
he kept pacing and walking around the city until he
could leave. One woman, a bright executive, became so
terrified and hysterical that she was willing to pay
a cab driver three hundred and fifty dollars to take
her on a two hour, 120 mile trip to Philadelphia so
she could be near extended family. There was another
woman, who prior to this flight to D.C., had not flown
for thirty years because of a long standing fear of
flying. Needless to say she became one of several who
refused to fly home. Some rented cars when they became
available. Others took the train. One couple even waited
for their son-in-law to pick them up in his long haul
truck. I ended up taking a plane (or in actuality, five
different short flights over a twelve hour period) to
eventually get back home.
On a positive note, despite the fact that the conference
participants were quite different from each other, our
shared, somewhat traumatic experience truly linked us
together. There is now a new kind of friendship among
most of the people.
I do not think the seriousness and the full sadness
of what happened on September 11th completely hit me
until I returned home. This leads me back to “Law
and Order”. Why does a show about criminals, police
detectives, and prosecuting attorneys so interest me?
I think the answer is quite simple. In this time of
major uncertainty with the World Trade Center disaster,
Anthrax scares, and increased general anxiety, it is
somewhat comforting to know that each night hardworking
detectives on the side of “good” almost
always apprehend the “bad” guys. If only
our world situation could be so uncomplicated.
[top]
Los Angeles Psychologist
July-August 2004
WHEN IS IT ALL RIGHT TO SAY NO?
I recently received an urgent page from a Mrs. Green,
the mother of a prospective patient (the names in this
article have been changed to protect privacy and conform
to standards of confidentiality). She was rather agitated.
She wanted her seven year old child seen right away
–he was not attending school, he was withdrawn,
he was pulling out some of his hair, and even slamming
his body against the floor on occasion. The school nurse
was apparently throwing out names of all kinds of possible
disorders for this child—including Asperger’s,
Autism, and Major Depression; these made the mother
even more frantic. I asked Mrs. Green how long she had
observed these behaviors. Except for the son’s
not wanting to attend school, the other cluster of behaviors
had been present for many months. As is my custom, I
asked Mrs. Green who had referred her, especially since
I do not see children that young. She indicated that
a major managed care company had given her my name.
I tried to tactfully tell her that I did not specialize
in working with young children and that I would not
be right for her son. She became outraged and shouted,
“You are the 5th person who has said this to me.
Don’t you like my insurance? Is it something I
said?” Then she abruptly hung up.
This article is written as an opinion piece that I hope
will generate some thoughts and further discussion.
It is not meant as a comprehensive document on the subject
of how to select (or reject) new patients. Some of you
might want to read or re-read contracts that you have
signed with various insurance/managed care organizations
and/or consult with an attorney regarding a clinician’s
rights and responsibilities in this matter.
While we all can empathize with the Green family, the
broader issue becomes what our responsibility or obligation
is regarding treating a patient who in a pre intake
“interview” on the phone presents as either
outside our expertise or as significantly more difficult
than we can handle in light of the demands of our other
patients. For instance, unless the psychologist specializes
in working with borderline personality disorders, how
many such patients can one reasonably have in an outpatient
practice? How do you handle the situation when a severely
depressed patient calls for an initial appointment and
based on your brief phone contact and your prior experience,
you believe that he or she should see a psychiatrist
for a medication evaluation first despite the managed
care company’s stating otherwise?
In informal discussions with several psychologists
who have been in practice for a number of years, none
seem to have a fully satisfactory answer regarding what
to tell prospective patients who for whatever reason
they feel uncomfortable in treating. The common response
that psychologists frequently give is that their caseloads
are full or that they are going away on vacation. I
know one psychologist who will tell a prospective patient
whom she does not want to treat that she has a 3-4 week
waiting list and even then the only time available for
an appointment would be around 10:00 am which is almost
impossible for many working individuals or students
to maintain on a regular basis. One senior psychologist
told me that he simply tells the prospective patient
that he “does not have the resources” to
handle the issues which are being presented. One psychologist
went so far as to say that for risk management issues,
he would not even return the call of the most severely
disturbed patient. He further stated, “If anything
happens to the patient before he gets to my office,
I do not want to be the one responsible”.
Obviously, for ethical reasons, I believe that it is
best to be truthful with the prospective patient about
why you cannot treat this person. I realize that the
patient might complain to the insurance carrier about
your “unwillingness” or lack of availability.
It is unlikely but conceivable that with enough complaints
of this type, one might be asked to resign from the
panel and thus lose a referral source.
Insurance companies have to share some of the accountability
for various psychologists’ being more selective
in whom they choose to treat. First, with some insurance
reimbursements being frozen at late 1980’s dollar
amounts, there is less incentive for psychologists to
want cases that most likely will require giving excessive,
unreimbursed extra time (often urgent phone calls) with
exceedingly tough patients and their families. Second,
some insurance companies do not always reimburse in
a timely manner and literally make the clinician jump
through hoops to get paid. Third, despite the fact that
clinicians take the time to fill out the recredentialling
forms listing the types of patients (by age, disorder,
or gender) that one is trained and experienced in treating,
often times the insurance company will give the patient
names of psychologists regardless of their specialty
(or stated unwillingness to treat certain patient types).
With all that the prospective patient sometimes has
to go through before he or she ever gets to your office
door, no wonder there is often great frustration.
What can be done to rectify these situations? Certainly,
we can choose to remove ourselves from all the panels
but that is not going to increase patient access to
care especially those deserving individuals who on their
own could not afford psychotherapy even at a reduced
fee. I look forward to more LACPA members volunteering
to educate and advocate for better healthcare for those
in our community while working to meet the professional
needs of psychologists. Further, it is hoped that LACPA
members will continue to work closely with our state
and national organizations to bring about necessary
reforms in the healthcare insurance industry.
In case you wondered what ever happened to Mrs. Green
and her son? I called her back and helped her find two
excellent child psychologists who not only were on her
insurance panel but were also available.
[top]
Los Angeles Psychologist
Nov/Dec 2000
“Original ideas:
- Internet 0
- Humanity 1,000,000,000,000,000”
This was part of an intriguing advertisement that I
recently came across for a company called PeopleSoft,
which links corporate e-business data to employees and
customers. Even the company’s name tries to downplay
its emphasis on new technology.
This concept was especially of interest since one area
in which I have devoted significant time this year has
been in helping to establish our organization’s
website and in planning how LACPA can become even more
technologically advanced in the coming years. With this
endeavor, I have given some thought to the impact that
the new technology and the Internet have on the pace
of our daily lives.
Earlier this year, I had the opportunity to attend the
annual American Psychological Association’s Convention
in Washington, D.C. where psychologist, noted author,
professor, and management consultant Randall White,
Ph.D. led a discussion on business life today. One top
information technology executive stated that the corporate
philosophy of the 1990’s included the phrase “Ready,
aim, fire”. But in the 2000’s the pace is
picking up even faster----“Fire, fire, fire”
with the understanding that if the company misses one
target towards a successful outcome, then the organization
is bound to hit another one as long as the pace is kept
fast…very fast. This philosophy was further expounded
by the now popular riddle about the three frogs on the
log. “If two frogs decide to jump off, how many
are left?” The answer is three, because none as
yet have acted on the decision.
Ms. Carly Fiorina, Hewlet-Packard’s chief executive,
in the July 24, 2000 issue of Forbes, expressed her
philosophy for the success of a big company, “Sharpen
your vision, focus and execution. Reimagine what you
can be. Work weekends.” Of course, not
all companies have this philosophy but in general more
individuals are working longer hours, with less time
allowed for extended vacations. Overall more stress
is experienced. Fun at work for many is now a distant
memory. Company loyalty is a rarity with job retention
a major concern for corporations today. Employees often
see themselves as working on an assignment and then
moving onto another project at another company.
Most of us will agree that the daily pace of our lives
has picked up significantly, possibly in part by the
demands of some of the newer technology. Just ask a
colleague how many e-mail, he or she has to sift through
upon returning from a vacation or conference or just
at the end of the day. Some of my patients are truly
wired for almost every eventuality—pagers, cell
phones, faxes in their cars, Palm Pilot schedulers,
and even digital cameras for almost instant transmissions
of pictures via their computers and the Internet. Corporate
life has either led the way or is reflective of this
“hurry up” trend in society.
Okay, in this my last column as LACPA President, I admit
it--I am guilty for moving LACPA further along in this
faster paced technological age. Our organization is
now getting e-mail from psychologists throughout the
country and from professionals in other parts of the
world. Such queries include questions about the state
of our profession locally and requests for Los Angeles
referrals or additional contacts.
While I have significant concern with the “speeding
up” of our society (of course, we can’t
totally blame the internet for that; Starbucks and other
purveyors of double espressos and lattes must share
some of the responsibility), this may, in actuality,
prove to be an ideal time for psychologists. We hear
so often about the decline of our profession, yet who
better to understand the emotions, behavior, cognitions,
and what motivates people than those in our profession.
We must be flexible as we move towards 2001 to use our
expertise to contribute to assisting our society in
a number of diverse ways, some outside the traditional
general office practice.As has been so well done during
this year in the LA Psychologist, several different
career paths or goals have been illustrated by those
who have already ventured into different areas, including
consulting, health psychology, geropsychology, community
psychology, as well as for some, obtaining psychopharmacology
training with the movement towards prescription privileges
authority. There are several psychologists who are working
in the area of Life Skills Training, which includes
a multi-modal approach with collaboration in the areas
of nutrition and exercise. As we look to the future,
how will telehealth play a part and what role will psychologists
have?
We need to be creative as we continue to find or maintain
that special niche for success and professional satisfaction.
And as we do, we need to take care of ourselves personally
as well. Wayne Muller, author of Sabbath: Restoring
the Sacred Rhythm of Rest, in the July 24, 2000 issue
of Forbes states that while “the world is speeding
up, some things aren’t built to run faster. The
human heart is one of them” He further concludes,
“It takes time for data to become wisdom.”
As this year draws to a close and thoughts move towards
holiday and family, I just wanted to take this opportunity
to thank everyone within the LACPA community for allowing
me the honor of serving as your President for this past
year. Special thanks go to our staff, our executive
administrator Patricia Fricker, our executive assistant
Carol Torcello, and our PRN resource assistant Melinda
Rothchild. Their steadiness and devotion keeps our organization
in a positive direction. I also want to thank the Executive
Committee (Helen Grusd, Jana Martin, Joe Grillo, and
Diane Siegel). Their support and hours of hard work
made my job so much easier. Finally, I want to thank
the LACPA Board as a whole, for their commitment to
psychology, our members, and to our entire community.
Take some time and have a wonderful holiday season.
[top]
Los Angeles Psychologist
Sept/Oct 2000
TALK TO AN EXPERT, FOR $19.95
Recently, I saw a new patient, let’s call her
Mrs. T., who had come in to discuss problems that she
was having with her husband who, according to her, wanted
sex all the time. She said that he kept quoting radio
talk show hosts Howard Stern and Tom Leykis, and she
was sick of this. She asked me what I thought of
Dr. Laura and before I could answer, Mrs. T stated that
she was a faithful Dr. Laura listener, even rattled
off Dr. Laura Schlessinger’s radio phone number
“1.800.DrLaura”, and in typical Dr. Laura
fashion, she indicated, “I am my kid’s Mom.”
Mrs. T. wanted me to know that she was very informed
about issues surrounding mental health and had even
instilled this in her children. She was, however, a
little concerned because her 17-year-old son was a regular
viewer of MTV’s Loveline and that the host Dr.
Drew was his hero. Mrs. T. went on to say that all they
ever talked about was “sex, sex, sex”.
My patient also stated that she was connected to the
Internet and proudly indicated that she got much of
her information from that source. She said that if she
had a problem, she would just log on to “Ask an
Expert, Ask a Friend” http://members.aol.com/biblprof/ask-expt.htm
and for the low cost of $19.95 per question, she would
always get feedback and would never feel lonely again.
She indicated that she knew that she could not always
get help from these experts. However she stated that
when she really needed more technical information she
would go to Dr. Koop.com http://drkoop.com. She was,
in fact, looking forward to attending a Dr. Koop sponsored
support group online later that day on “stress
management for parenting.”
Mrs. T was not even sure that she wanted to come to
an office for psychotherapy. When I asked her why she
made this first appointment, she indicated that she
was tired of being on hold for Dr. Laura. In desperation,
she had even tried unsuccessfully to get through to
another Talk Radio host Dr. Toni Grant.
Her husband was reportedly upset that she had made the
appointment. After all, he had told her that if they
couldn’t work out their marital difficulties themselves,
they could always “Ask Your Sex Therapist”
http://www.mindspring.com/~debfox/sexask.html. For only
$25 for each question, this was certainly less expensive
than a psychologist office visit.
As Mrs. T. talked on and on about her total trust for
these radio personalities and Internet self-helpers,
I noticed that she was becoming more and more manic.
Further, she revealed that at times she was very depressed.
I even suggested that she might also want to see her
family doctor or a psychopharmacologist for a medication
evaluation. She said, “Oh, no…there is a
new book called Prozac Backlash (referring to Prozac
Backlash: Overcoming the Dangers of Prozac, Zoloft,
Paxil, and Other Antidepressants with Safe, Effective
Alternatives by Joseph Glenmullen). I can’t take
anything like that.” When I asked her what she
had learned in reading this book, she indignantly said,
“I didn’t actually read the book, but I
know it is a best seller on Amazon.com. If I take anything,
it would be Remeron because I saw this neat site on
the Internet when I was searching for information on
depression.” (Unfortunately, Mrs. T. may have
been unaware that a pharmaceutical company had sponsored
this site on depression http://www.depression-net.com.)
After she left the session, I was intrigued to find
out more about some of her other Internet references.
Apparently, some of these so-called authorities from
“Ask an Expert, Ask a Friend” are not licensed
psychotherapists. One received his master’s degree
in the area of Human Resources and is in the ministry.
Another loves fishing and the outdoors.
In addition, while Dr. Laura states that she is not
a psychologist but a Ph.D. in Physiology with a Marriage
Family Therapist license, the average listener cannot
distinguish the difference. Further, when she talks,
people listen. While her anti-gay position is quite
disturbing, her views on the importance of family values
seem to resonate with people across the country. According
to RadioDigest.com, nearly 20 million people listen
to her each week. Those that do listen begin to believe
that all problems can be solved in 60-second sound bites.
Then they question why their own psychologists aren’t
helping them solve their problems as quickly.
Through the increasing popularity of talk shows and
websites, which focus on mental health issues, it is
obvious that the public wants more of this kind of information
and related services. Paradoxically, it seems that while
more people have access to information, what they often
come away with is material that is either superficial
or not fully understood. Chris Peck, Editor of the Spokane
Spokesman-Review, in a speech given at the Pew Center
for Civic Journalism Convention in August 1999, indicated
that twenty-five years ago, 70 percent of adults read
a newspaper regularly. Today, 51 percent read the paper
regularly. Five years ago, less than one in ten American
households had access to the Internet or ever went online.
Today, over 50 percent of Americans have access to the
Internet. Further, the number of people who sign on
regularly, as in the last 7 days, is doubling each year.
Clearly, as more people are becoming Internet savvy,
more and more self-help sites are being accessed, with
no mandated guidelines as to their quality or to the
competency of their creators. We as psychologists need
to get out of our offices more, talk to the media, and
in some instances become part of the new media. Further,
we must be willing to take action against those who
are trying to make money off of the unsuspecting consumer.
As we embrace the new technologies, we also need to
be the ones providing more of the information and in
a manner that can be fully understood by the general
public. The American Psychological Association has recently
launched an excellent source of consumer related material
on a wide variety of mental health related topics, everything
from “Dealing with Anger” to “Nine
Tasks for a Good Marriage” http://www.helping.apa.org/dotcomsense/.
Now if I could only convince Mrs. T. to explore that
website.
You may have wondered what finally happened to Mrs.
T. I suggested that she return for a follow-up appointment
the following week at 3:00PM but she declined. “I
can’t do it then, Oprah’s on and next week
is, How to solve your relationship problems in 5 easy
steps.” Oh, well maybe another time.
[top]
Richard Sherman, Ph.D.
The California Psychologist
September/October 2007
A Special Thing Happened on the Way to Writing this Article
In keeping with this issue’s theme of Leadership, I was planning on writing an article on the current state of health care in our country and how we need psychologists as proactive leaders to work towards crafting, advocating for, and implementing a new strong two pronged private-public healthcare system that guarantees basic medical and psychological care for all our residents. In the model that I envision, I also anticipate a dynamic primary role for psychologists including diagnosing, treating, and prescribing as well as directing programs.
However, a most interesting situation developed as I was about to write this column. I was appointed to be a member of the CA Board of Psychology. In 2003, when Governor Arnold Schwarzenegger won the recall election, I had applied for a non-paid Board appointment. This short list included the Board of Psychology. At that time, except for an acknowledgement letter, I never heard further. A few months ago, I unexpectedly received a call from an assistant appointment secretary from the Governor’s office. He asked if I still wanted to be considered for an appointment to be a member of the Board of Psychology. I was requested to update my application and participate in a phone interview shortly thereafter.
It was not until late June that I received word that I had been selected to join the Board of Psychology as a psychologist member for a three year term with the first meeting to be in early August. I accepted this appointment for which I was quite humbled and honored. Serving on the Board will afford me the opportunity to honor one of my personal and professional pledges, that of service to our communities. In this instance, I will work to protect the safety and welfare of consumers. In so doing, I will bring to the Board my unique perspective based on thirty years of experience as a psychologist and my extensive participation in and knowledge of organized psychology.
Timing of course is never perfect and my only regret was that in order to avoid even the perception of a conflict, I had to step down as your CPA President in the middle of July. The good news is that CPA is blessed with excellent, solid, and compassionate leadership. I am so pleased that Dr. Miguel Gallardo, who was President-Elect during my term and has a long history of service to CPA and APA, has now become CPA’s President. He is working with CPA’s strong team of officers-Drs. Gilbert Newman, Betsy Levine-Proctor, Sandra Harris, and Dean Haddock, a dynamic Board of Directors, an exceptional Executive Director Dr. Jo Linder-Crow, and a wonderful CPA staff.
I am so proud of what CPA accomplished during my watch, including being named outstanding state psychological association, and I will look forward to CPA’s continued growth and success. I plan to remain an active member of CPA and I look forward to seeing you at many CPA functions in the upcoming months.
[top]
Richard Sherman, Ph.D.
The California Psychologist
March/April 2005
Confessions of a Recovering Managed Care Provider
The following was conveyed to me by a psychologist
colleague, Dr. Tom W. (not his real name), who has been
in private practice for over twenty-five years. He has
seen his practice go from one that is primarily fee-for-service
based to one largely impacted by managed care. Here
are his thoughts, impressions, and trials and tribulations
as he extricates himself from the influences of managed
care:
I became a provider for a number of managed care organizations
(MCO’s) when they first entered the California
market place in the 1980’s. At the time, managed
care was touted as the wave of the future. There were,
in theory, several advantages for both the patient and
the clinician. For the patient, there was promised easy
access to qualified providers along with reasonable
fees and co-pays. For the provider, the MCO marketing
was akin to, “Focus on quality patient care and
let us handle all the administrative functions. Moreover,
for seeing patients at a ‘slightly’ reduced
fee, you essentially will be guaranteed a steady stream
of patients”. The hospital where I worked encouraged
my participation and most of my colleagues were scrambling
to sign up for as many panels as possible. The ominous
side was the strong portent that if we did not sign
up, eventually there would be limited access to prospective
patients.
In fact, in the early 1990’s, there were several
multi-disciplinary groups that were being formed and
competing with one another to actually negotiate contracts
with the managed care organizations. In retrospect,
it seemed like the actual motto of several MCO’s
was the following, “We give you the patients,
we make most of the profit, and you do all the work---staffing,
quality improvement, peer review, marketing, risk management,
and so forth”. These were, in a sense, often clinics
without walls. An incredible amount of unnecessary paperwork
was generated. For instance, I would see the patient
in my office, prepare a bill which was faxed to the
group’s central office (usually the psychiatrist
or psychologist director), then a new bill (almost identical
to the first bill) would be generated which in turn
was submitted to the insurance company. For all that
“service”, an additional 20% was deducted
from my already reduced rate!
Fortunately these multidisciplinary groups, as configured
for the MCO’s, for the most part have disappeared.
Still I found myself on many managed care panels. In
fact, recently, I saw patients whom I thought had private
insurance and later found that my reimbursement rate
had been decreased because their plan was connected
to some obscure MCO which still had me on the list.
To make matters even more complicated, several of the
smaller MCO's have merged over the years and changed
names without bothering to notify the psychologist providers,
even though they are, at minimum, supposed to keep current
malpractice insurance and license information on file.
I rationalized remaining as an MCO panel provider for
several years. I did and still do believe that I was
helping patients who might otherwise not be able to
receive quality mental heath care or any care, for that
matter. I sensed that my clinical documentation may
have improved somewhat because I knew that I might be
subjected to periodic concurrent chart reviews (I was).
From being a member of an MCO Peer Review Committee,
I saw first hand how much emphasis the MCO placed on
providing urgent and emergent care in a timely manner.
(The company may have just been protecting their own
interests but in a true crisis situation, clearly the
patient was the beneficiary.)
But finally over the years, I have painfully learned
that the concessions that the psychologist must make,
and the professional denigration that one who works
in the MCO setting has to endure, is just too high.
There is often a contradiction in the verbiage of the
MCO’s. One MCO recently wrote me and stated that
one of its goals is “to help your patients remain
engaged in treatment until they experience optimal benefit.”
However, this is the same company that informs the patient
that they have 30 visits per year (somehow there is
a loop hole so these patients do not qualify for parity
regardless of diagnosis). Yet, after 12 visits, the
MCO often initiates the arduous process for the clinician
of having to justify each additional visit. Clearly,
with most MCO’s, the psychologist has to change
the way he or she practices, with emphasis on referral
for medication, reliance on community services, and
overall reduction in intensity of care.
Further, there is the self-criticism that one may experience.
While the MCO executives continue to get huge salaries
and bonuses (e.g. over $12,000,000. for the head of
Aetna), the psychologist is still caught in a time warp
with reimbursement fees mostly frozen at 1980’s
rates, which were discounted and low even then. Most
managed care patients have their insurance either through
their own employment or through that of a family member.
While the incomes and benefits of most employees have
risen over the years, these patients are often unaware
of the low rate of reimbursement that the psychologist
receives.
Despite the myriad of negatives, a large number of psychologists
will continue to see almost exclusively managed care
patients. They do this for many reasons, some noble
and some because of the uncertainty of having to develop
new career opportunities. Sadly, they become beholden
to mega-structures that see the psychologist mostly
as a provider number and as a profile on a computer
screen.
So what is a psychologist to do? The path is not always
clear, especially since anticipated changes in health
care delivery will ultimately affect clinicians in both
the private and public sectors. And as of this writing,
one does not know what the Federal government might
eventually propose especially in the area of more mandated
health care benefits for seniors and young children.
Recently, there has been a positive thrust for psychologists
to interact more and become more integrated into health
care in general. This has definite benefits for the
patient given that utilization of mental health services
can often prevent or lessen the impact of many diseases.
According to a recent article in Behavioral Healthcare
Tomorrow (December 2004) entitled “A New Frontier:
Psychologists Practicing in Primary Care Settings”,
psychologists Reich, Romano, and Kolbasovsky indicate
that primary care physicians treat nearly 75 percent
of patients who are seen for depression. Further, close
to 50 percent of medical patients fail to follow through
on mental health referrals. This improves significantly
when the behavioral health specialist is seen as part
of the health care team, especially when the psychologist
is “co-located” in the primary care setting.
As a profession, however, we have to be wary regarding
what the insurance companies are doing as they “support”
this trend towards integration of services. Aetna recently
bought back its mental health division from the now
bankrupt Magellan Health Services and will no longer
have a major mental health carve-out company to provide
services to its members. So far so good? One of the
results of this change according to William Popik, MD,
Aetna’s chief medical officer, as reported in
amednews.com (12-27-04), is that key to the new approach
will be opportunities for primary care doctors to have
a greater role in diagnosing and treating patients with
psychiatric/behavioral health problems. Unfortunately,
Aetna appears to wants to reduce the role of psychologists
and psychiatrists even further.
In his last words about his journey to recovery, Dr.
W. concludes, “I am in the early post managed
care phase of my professional development. I am working
on creating a niche, being creative, and getting out
there and letting people know what I can do….
Everything has become simplified. I no longer feel that
there is a third person (the Managed Care representative)
in the room when I do therapy. Less time and energy
is spent on bureaucratic paperwork. Billing and getting
paid is actually easier. With more time available, I
happily see some low fee patients and even have more
time for my family…I will keep you posted. ”
[top]
Richard Sherman, Ph.D.
April 17, 2003
The California Psychologist
July/August 2003
ALICE IN HIPAA LAND
WARNING: The following is not intended to help the
reader become HIPAA compliant. Nor is this article intended
to review the multitude of HIPAA products and services
that are being promoted and advertised, more and more
each day. Rather this is a summary of a discussion that
I had with a trusted colleague who shared her frustration
in trying to prepare her individual practice for the
recently implemented HIPAA rules.
I had thought that I was going to have a dialogue with
Dr. Alice Sommers, (not her real name), but I quickly
began to sense that I was either listening to a Dennis
Miller rant or had stepped back into the upside down
world of the characters in Lewis Carroll’s Alice
in Wonderland.
Alice was more frustrated than I had ever seen her.
She stated, “ I am HIPAAed UP. I have attended
several lectures on HIPAA and I still don’t understand
everything. Even the experts can’t agree. I feel
like I’m at the Mad Hatter’s Tea Party with
everyone arguing and nobody making any real sense. And
the forms people are selling. What kind of standard
is this if some Treatment Consent forms are only one
page, others are three pages, and I saw one that was
eight pages in length? And then we have to have a Notice
of Privacy Policies and Procedures. These will add another
three pages at least. How can I give my patients all
these documents and expect them to read them, let alone
understand them? My patients can alter or halt the agreement
with me at any time but how can I explain all the ‘legalese-like
terms’ such as binding, ‘in reliance’,
and revocation? Some of these forms have just too many
‘thereofs’ for my comfort. There is just
not enough time before, during, or after the sessions
to help the patients understand all their rights, especially
when these regulations are still subject to interpretation
and change.” Alice was inconsolable. When I tried
to mention that all we were expected to do was strive
for reasonable compliance, she escalated even more.
She had taken the APA online course and had tried as
best she could to adopt the forms provided for her practice
and to comply with California privacy laws. She did
expound, “The course was pretty good but the forms
were just too complicated.” She screamed out,
“And when I try to simplify these forms, how do
I know that I am not losing some of the important points
that are supposed to be in the documents.”
Then she brought up an interesting point. Alice is trilingual.
She has patients with whom she communicates in a number
of languages. She yelled out, “How are my patients
for whom English is not their primary language ever
going to understand all of this?” as she pointed
to the forms. She went on to say, “I barely understand
the material myself. I just don’t have the time
or knowledge to translate these into Spanish or Russian.
What am I to do? I feel like I followed the rabbit down
the hole—I just can’t get a handle on things—either
I’m too large to get through the door or too small
to reach the key.”
I tried to console Alice. But she remained distraught.
“I’ve been treating patients for over twenty
years. Now all of a sudden, my patients are going to
come in and amend their records. Who is going to sit
there with them as they review their charts and who
is going to pay for that? Even with separate Psychotherapy
Notes, am I going to have to pre-censor everything I
want to write? I know the goal of HIPAA is to employ
safeguards to protect the patient but what about us?”
Again, she referred to the other Alice. “Sometimes,
I am afraid that the Queen of Hearts is going to have
me beheaded if I make even a small mistake.”
Again I tried to calm her but I don’t know if
she was listening. I wanted her to know that Division
I has a number of excellent psychologists who are well
versed in HIPAA Compliance, in particular, Drs. Dean
Given and Bram Fridhandler. We are also very fortunate
at CPA to have someone of Dr. Charles Faltz’s
caliber as Director of Professional Affairs. He has
followed HIPAA and the changing regulations and interpretations
from the beginning. I also wanted her to realize that
even though HIPAA compliance was technically required
April 14th, 2003, CPA would be sponsoring additional
workshops on HIPAA and related topics to further assist
members in the coming months.
Finally, at Alice’s request, I glanced at the
forms she had prepared and on first review, they looked
reasonable. She was relieved at my response. As we parted,
I thought I heard her say in a booming loud voice, “In
the words of the White Rabbit, HIP HIPAA HOORAY!!”
No, I must have misheard her.
[top]
May/June 2003
Reality TV and the New Breed of Patient
On a recent evening when I could watch only so much
Iraq and terrorism coverage, I began to consider what
other television “entertainment” options
there might be. It quickly became obvious that traditional
television has been replaced by a new breed of programming
that includes a plethora of so-called reality shows,
an inundation of nonstop news coverage, and a variety
of self-help shows that all masquerade as entertainment.
Just flip through the TV Guide for a glimpse of these
new trends. One could tag along with a group as they
return to their “High School Reunion;” learn
from Oprah the secret to a happier life; or “Talk
Back Live” on CNN’s current affairs show
that solicits the opinions of its television viewers.
You might ask how this relates to a column geared for
psychologists in professional practice. Stay tuned.
Our fascination with reality programs is not only coupled
with our quest for entertainment but also for our search
for the most up-to-date information. Most television
stations cater to these demands. For instance, one local
Los Angeles television station now delivers six hours
of news per day. For those who have cable, CNN has two
full time competitors and C-SPAN, which carries live
coverage of Congress and related political events, has
now grown into three different stations. And with the
Internet, one can have almost instant access through
“streaming” news and related information.
The trend towards our wanting to “be there”
for world and life changing events started gradually
with the live coverage of the events surrounding the
assassination of President John F. Kennedy and has continued
to the present with almost nonstop coverage of the aftermath
of 9-11-01. We have seen this again most recently with
the tragic loss of almost 100 people in a devastating
fire at a Rhode Island nightclub. Today we also want
to be “there” for less global news events.
The activities of Michael Jackson, the Robert Blake
case, and the disappearance of Laci Petersen, the missing
pregnant woman from Modesto, CA, have captivated a large
number of people who watch intently for the latest news.
What this over-saturation of reality television programming
allows us to see up close is raw human emotion, such
as the bravery of families in light of tragedy and even
the flaws of everyday people.
What does all this say about the client or patient
we might see in psychotherapy? It seems undeniable that
the new breed of television programming has resulted
in a new breed of patient. We must be willing to address
the implications of this. For one, our patients who
watch any of the self-help shows are becoming increasingly
“more sophisticated” in the knowledge they
bring into our sessions (“Well, Dr. Phil said…”).
Some may even feel more empowered to do something about
the very situation that brought them into therapy. Recommended
by authors on programs such as the Today Show, our patients
are often more aware of the latest “lay”
books on divorce, relationships, and child rearing before
we are. Often even our patients who choose not to partake
in the reality television frenzy are affected by the
changes evident on television. For instance, there has
been an increase in the pharmaceutical advertisements
that target consumers directly such as with Paxil, whose
slogan claims, “Your life is waiting!” Our
patients may also question more. They may look you up
on the Internet via Google to see if you have a website
(and its quality), where you have been quoted, and what
other professional activities you have pursued.
The recent inundation of news coverage also has implications
for the new breed of patient. We live in a global community
where communication about news events is often transmitted
in seconds. Our patients are part of this larger community.
They connect in ways that were not possible years ago.
For some they may become quite emotional as they watch
these events (such as 9-11, the war in Afghanistan,
Iraq) over and over. They might become even overly invested
in the sad drama of another family hundreds of miles
away. Laci Peterson becomes like their sister or daughter.
While many of us are still providing individual psychotherapy,
we must now deal with the trend toward collective emotions—generalized
anxiety, “group” depression, and traumatic
stress.
All of these changes may prove challenging to the
clinician who now must deal with this new breed of patient.
While we may not be able to keep up with all of their
knowledge of the news or of pop culture (or some of
us may not even want to try), we still need to help
them work through the issues that initially prompted
them to seek our assistance. We want to help them explore
what might be missing on a day to day basis—including
meaningful relationships, family closeness, the striving
for good health-both psychological and emotional, spiritual
awareness, and renewed happiness, even in difficult
times. As we work with these patients on these and other
issues, they may even have less need to tag along with
Joe Millionaire as he wines and dines women throughout
Europe or traipse along the Amazon with some of the
Survivors.
[top]
December 2000
Meeting with Vice President Al Gore
I recently had the opportunity to participate in a
round table discussion with Vice President Al Gore.
How this came about is truly reflective of the wonderful
networking and lobbying that CPA has done for so many
years.
State Senator Liz Figueroa (D-Fremont) who considers
CPA a very positive organization and resource recently
had a bill passed which works towards increased protection
of patient records and information contained in those
records (Senate Bill 19). One of Vice President Gore’s
themes is protecting consumers from having their confidential
information released, or worse, sold to other organizations
without their consent. He considers Senator Figueroa’s
legislation a strong one and would like to see other
states adopt California’s law.
I have learned that in politics, events can happen quickly
and with little notice. On Monday Sept.18th, I received
a call from John Van Etten of CPA that Liz Figueroa
was going to be part of a meeting with Vice President
in Los Angeles the next morning at a small school for
disabled children. John asked if I or another psychologist
would be able to attend.
When I arrived at the school, I quickly learned that
I was part of a very small group that was meeting with
the Vice President to discuss the issue of protecting
patient records. This dialogue was to occur before Vice
President Gore was to hold a town hall assembly on the
same topic. He wanted to integrate parts of our discussion
in that larger meeting. To my surprise, there were only
about fifteen people at this roundtable discussion,
with no cameras and no reporters. Just the Vice President
and us! There were only a small number of medical people
and an even smaller number of mental health professionals.
While at the meeting I got the opportunity to meet again
with Mrs. Sharon Davis, Governor Davis’ wife.
Mrs. Davis seems very committed to the expansion of
mental health services. As a matter of fact, last June,
several members from the LACPA’s Governmental
Affairs Committee, in collaboration with CPA, had a
lobbying day in Sacramento. Through the efforts of Dr.
Dana Kiesel, Chair of LACPA’s GAC, we met Mrs.
Davis and discussed several of our political issues.
Also in attendance was Assemblywoman Sheila Kuehl (D-41st
Assembly District) of Santa Monica.
I cannot emphasize enough how important CPA’s
lobbying efforts are especially in building relationships
with our elected officials. Since Vice President Gore
was a little late, we all were “confined”
to a small classroom in anticipation of his arrival.
The additional time gave us the opportunity to listen
and chat with these state leaders in a way that is rarely
possible. Those of you who have participated in a Lobbying
Day know how precious the time we get with a legislator
is.
Of course, the main event was meeting Vice President
Gore who seemed genuinely interested in listening to
the experiences and impressions of those in the room
regarding the issue of protecting the privacy of patient
records. He seemed very disturbed that information contained
in patient records is apparently being sold. A woman
shared how when she first became pregnant, only her
physician, the lab that ran the test, and the pharmacy
where she had earlier purchased a home pregnancy test
knew anything related to the possible pregnancy. Yet
a few weeks later, she received samples of baby bottles.
We shared with Vice President Gore that some prospective
patients are afraid to even access their insurance for
psychotherapy because of concern that the insurance
companies will not maintain the absolute confidentiality
of the material that they request in order to case manage
and to process the claims. Vice President Gore responded
by stating that he believed that the insurance companies
are requesting too much information and when all is
not received, this gives them a rationale to hold back
payments. Vice President Gore seemed sincere in his
comments and in his interest to gradually make reforms
to the current insurance system.
In summary, this special experience with Vice President
Gore and some of our state officials would not have
happened without CPA members networking with our legislators.
Liz Figueroa called CPA because she feels comfortable
with our state association. This reaffirms the importance
for all CPA members to support the lobbying efforts
by our state organization. Through continued networking
and lobbying, CPA’s voice will be even stronger
in Sacramento.
Dr. Sherman has a private practice in Southern California
and is a Member of the Board of Directors of Division
I and is currently President of the Los Angeles County
Psychological Association.
[top]
 |
| |
 |
Richard with Dr. Pat DeLeon,
Past President of APA |
| |
 |
Richard meets Vice President
Al Gore at a Town Hall Meeting |
| |

|
Richard visits with psychologist-legislators
at a CPA PAC Dinner |
| |
 |
Richard meets with Governor Schwarzenegger |
| |
 |
"Just for fun", Richard
meets Rupert from the David Letterman Show. |
| |
 |
Richard at Old Executive Office Building in Washington, D.C. |
| |
 |
Board of Psychology Swearing in Ceremony |
| |
 |
Richard and Insurance Commissioner Steve Poizner |
| |
 |
Richard at KABC Radio Studio |
| |
 |
Richard meets President George Bush |
[top]
|
|
| |
|
|
|
|